
February 22, 2017
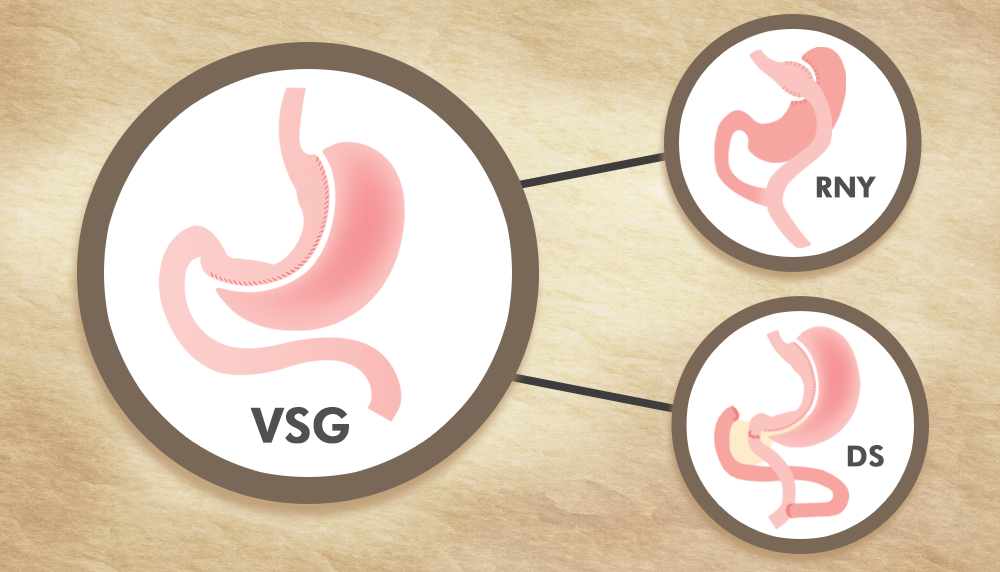
The Vertical Sleeve Gastrectomy (VSG) is rapidly emerging as among the weight reduction surgical treatment treatments that patients select one of the most. For some bariatric cosmetic surgeons and patients, the VSG has replaced the Proximal Roux-en-Y (RNY) Gastric Bypass as the most popular weight loss surgical treatment currently done.
Elimination of the upper external stomach – the primary source of ghrelin (cravings stimulating hormonal agent) production and pylorus preservation supply a more natural gastric restriction than the RNY or the adjustable gastric band (AGB). Many patients lose about 50-60% of their excess weight (%EWL) – very little different from what is typically reported after the RNY after five years.
Unusual Weight Gain
Historically, about 25% of gastric limiting surgical treatments, of which the Sleeve Gastrectomy is a prime example, might eventually need a revision to a different class of weight reduction surgical treatment. In spite of using a repaired size bougie, there are boundless variations to how the Sleeve is created and this results in a variable geometry/ stomach capability a few years out.
One of the initial steps in evaluating a client who has either not lost appropriate weight (specified as less than 50% of their excess weight) or has regained a substantial amount of weight after a VSG is to identify – has the surgery stopped working the patient or the patient stopped working the surgery?
The pyloric valve is naturally created to hold back strong foods such as protein and leafy green veggies – foods that were all placed on the world for us to endure. The VSG depends on this valve for feedback and weight loss outcome revolves around the patient understanding this concept and utilizing it to its maximum capacity.
However, the majority of the “foods” that we consume – such as liquids (including liquid calories), soft mushy foods, etc, bypass the pylorus. Offered our busy lives, if a patient’s staple diet is controlled by these foods, then gradual weight restore is inescapable and this has little to do with the operation. When the clinician figures out that credibility of the patient elements contributing to weight restore, the next step is to evaluate the anatomy and performance of the VSG.
Premises for a Modification of the VSG
Creating a VSG brings the naturally stretchable upper portion of the stomach (the fundus/body) in direct proximity to the muscular lower part of the stomach (the antrum) that does not stretch very much. Over time, regardless of the best efforts of the cosmetic surgeon and client, the upper half (or 2/3rds) of the sleeve can dilate substantially. This can be assessed by carrying out an upper gastrointestinal (UGI) endoscopy – which allows the surgeon to “look” inside the food pipe (esophagus) to check for reflux, the stomach residue to get an idea of the size, both the upper and lower halves of the VSG, acquire tissue samples (biopsies) to check for pre-cancerous modifications (Barrett’s esophagus) and bacteria that might cause ulcers (Helicobacter pylori or H. pylori).
The next phase of the evaluation is to inspect the practical elements – patients would consume a quantifiable strong meal – e.g. garbanzo beans, hamburger, egg salad, etc, blended with some barium (sorry!) till they feel complete and they would be evaluated by a radiologist using an upper gastrointestinal (UGI) fluoroscopic research study (barium swallow) to evaluate how much a client can eat before they feel full (in ounces) and how does the stomach remnant look when it is distended maximally – simply put, its geometry.
Many patients with a properly created Sleeve would feel complete after 4-5 oz of solid food. Anything in excess of this, together with an outstretched upper part of the Sleeve is grounds for modification of the VSG.
Depending on the client’s disease concern (excess weight above perfect body weight), weight loss expectations, clinician’s assessment of the client’s post-surgery compliance with dietary supplements, transforming the VSG to a malabsorptive operation such as the standard Duodenal Switch (DS) or the more current variation of the DS – Duodenal Change Single Anastomosis (DS-SA) may be necessary.
These operations involve a transection of the duodenum just beyond the pyloric valve and redirecting the food to the lower half of the intestinal tract (the “alimentary limb (AL)”). The upper half of the intestine does not enter contact with the food but serves to divert and dilute the digestion juices (bile and pancreatic juice) (the “biliopancreatic limb (BPL)”).
Absorption of calories and nutrients is confined to that section of the AL that enters contact with the watered down digestive juices (the “typical channel (CC)”). This develops a “ceiling” on the amount of calories that can be taken in daily which provides for about 20% much better weight reduction (i.e., about 70-75% EWL) than what can be typically accomplished with a stomach limiting surgery such as the VSG.
Diabetes remission rates are reported to be ~ 90% after the DS/ DS-SA.
Directing the food into the lower half of the intestine promotes secretion of hunger reducing hormonal agents such as PYY (polypeptide YY) and GLP-1 (glucagon-like peptide 1) which play an important function in much better weight loss, weight upkeep and diabetes control.
Taking Additional Nutritional Supplements are Needed
Among the inescapable repercussion of this anatomy is that clients require to be certified about taking additional dietary supplements – protein, vitamins (especially fat-soluble vitamins – such as Vit D, A & E), Vit B12, calcium citrate, iron, zinc etc to decrease the threat of medically significant nutritional deficiencies. They should also be compulsive about obtaining security laboratory studies and follow-up with the clinician. Diverting food from the proximal portion of the intestinal tract (duodenum and jejunum) areas which are naturally created for effective absorption of certain nutrients such as iron, calicum, and Vit D, increases the threat for anemia, bone loss (osteopenia and osteoporosis) and kidney stones.
Preserving sufficient core muscle strength and muscle mass by keeping an active life-style, weightlifting, staying well hydrated etc would be the very best method to mitigate this problem. Reducing the small digestive direct exposure to food does carry some adverse effect – such as gas, frequent stools and odor problems – thought to be from bacterial breakdown of partially absorbed food within the large intestine or colon. These issues are typically connected with usage of carbohydrate abundant foods. Most of these malabsorptive symptoms get better with time as clients adapt to the malabsorption and can be controlled with over-the-counter items. Choosing an operation such as the DS-SA variation which has a longer CC (10feet vs 5 feet with the conventional DS) can decrease these issues without substantially affecting the short-term outcome.
Gastro-esophageal Reflux Illness (GERD)
GERD signs consisting of heartburn, reflux, difficulty swallowing and keeping down strong foods can happen in ~ 10% of VSG patients. While in the huge bulk of patients these symptoms improve over time, in some they do not in spite of being on proton-pump inhibitors (PPIs) such as omeprazole and other acid-reducing medications.
GERD signs can result occasionally result from mechanical problems related to either a mechanical issue within the Sleeve or a pre-existing hiatal hernia. This is a common condition (affects practically 20% of the basic population) where the union in between the stomach and the esophagus happens above the diaphragm (an umbrella shaped muscle that separates the chest from the abdominal cavity). The esophagus or food pipeline passes through a hole (“hiatus”) in the back portion of this muscle to join the stomach normally rather of listed below the diaphragm.
While a lot of clients with a hiatal hernia do not have symptoms, in some, particularly after they have actually had substantial weight-loss, it might possibly be the cause of GERD/ GERD related symptoms. This can be resolved by laparoscopic hiatal hernia repair.
As discussed earlier, the VSG residue stomach tube – has a natural angulation about midway in between the lower esophageal sphincter (LES) (or the upper stomach valve at the bottom of the esophagu) and the pylorus (lower stomach valve). This is the watershed zone (called the “incissura” of the stomach) in between the more easily distensible upper portion of the stomach tube (the “fundus” and “body” of the initial stomach) and the less distensile lower part of the stomach (the “antrum”). The stomach tube is naturally bent at this area. This is what produces a natural angulation within the stomach tube which typically does not trigger an issue. Rarely, this may be the website of a repaired obstruction or stricture which may require to be addressed by a UGI endoscopy with endoscopic balloon dilation. Absence of action to these conservative techniques might necessitate a modification to a Roux-en-y (RNY) gastric bypass. Typically most of these are Proximal RNY gastric bypasses. This usually includes dividing the stomach tube about a couple of inches below the gastroesophageal (GE) junction or LES(where the esophagus joins the stomach) to produce a small stomach pouch. The upper intestinal tract (called the jejunum) is then divided about a foot from where it comes from (thereby developing a short BPL). The bottom end of the divided intestine (called the Roux limb) is then linked to the stomach pouch. The brief BPL is then connected to this Roux limb about 5 feet downstream to develop a long (usually not determined) CC. This operation is usually related to a ~ 50% medium-term EWL and has some threat for weight gain back (as is typical of all stomach limiting surgical treatments)
Malabsorptive RNY GBP (MGBP)
Under certain situations, depending upon the client’s disease problem (e.g., h/o Super Weight problems i.e., initial BMI > 50 or Super-Super Weight problems i.e., initial BMI > 60) and associated co-morbidities (e.g., diabetes) we could create a malabsorptive RNY GBP (MGBP) with a long BPL, a ~ 10 ft AL and short (normally 5-7 feet) CC. These operations (similar to all malabsorptive operations) are related to a 70-75% EWL with a lower danger for weight gain back.
As a basic rule, all revisions do carry a higher threat for problems such as leaks, infections, bleeding and medical issues such as embolisms development in the legs (deep vein thrombosis) or lungs (pulmonary embolism). It is necessary to for that reason pick a bariatric surgical practice that has actually established a good track record in carrying out complex revisions.
Comprehensive assessment and proper revision surgical treatment can address these problems successfully and restore health and lifestyle.
Are you thinking about a VSG Modification? Dr. Myur S. Srikanth discusses revising to a RNY or DS.





